

What PTSD Really Looks Like
A Day That Refuses to Stay in the Past
Marcus was a 38-year-old high school teacher. To his colleagues, he was the calm one, the one who always had a steadying word for a distressed student, the one who stayed late to grade papers and was first in the classroomeach morning.
What they did not know was that Marcus had not slept through the night in two years.
It had started after a car accident on a wet highway, a collision that lasted less than three seconds and left him physically unharmed. Yet something had shifted. A truck backfiring outside the school gymnasium could send his heart into a sprint he could not explain or slow down. He stopped driving on rainy evenings. He withdrew from the Friday evening dinners he used to love. He told himself he was simply tired, that anyone would feel this way. He told himself it would pass.
It did not pass.
Eighteen months later, Marcus sat in a doctor's office and heard four words he had not anticipated: "You have PTSD."
His first response was disbelief. PTSD, he thought, was for soldiers who had returned from combat zones. It was not for teachers who had walked away from a car accident without a scratch. It was not for him.
"PTSD, he thought, was for soldiers. It was not for someone like him. He was wrong."
Marcus is not a fictional extreme. His experience reflects the reality of millions of people who are living with post-traumatic stress disorder and do not yet know it, or who know it but carry the weight of a profound and persistent misunderstanding: that PTSD is something that happens to other people.
It is not. And the first step toward healing, for Marcus and for anyone, is understanding what PTSD actually is.
What PTSD Is and What It Is Not
Setting the Record Straight: Myths and Facts
Post-traumatic stress disorder is one of the most misunderstood conditions in mental health. Persistent myths about who it affects, what causes it, and what it means about a person's character continue to delay diagnosis, discourage help-seeking, and compound the suffering of those who experience it. The following facts are drawn from authoritative clinical and public health sources.
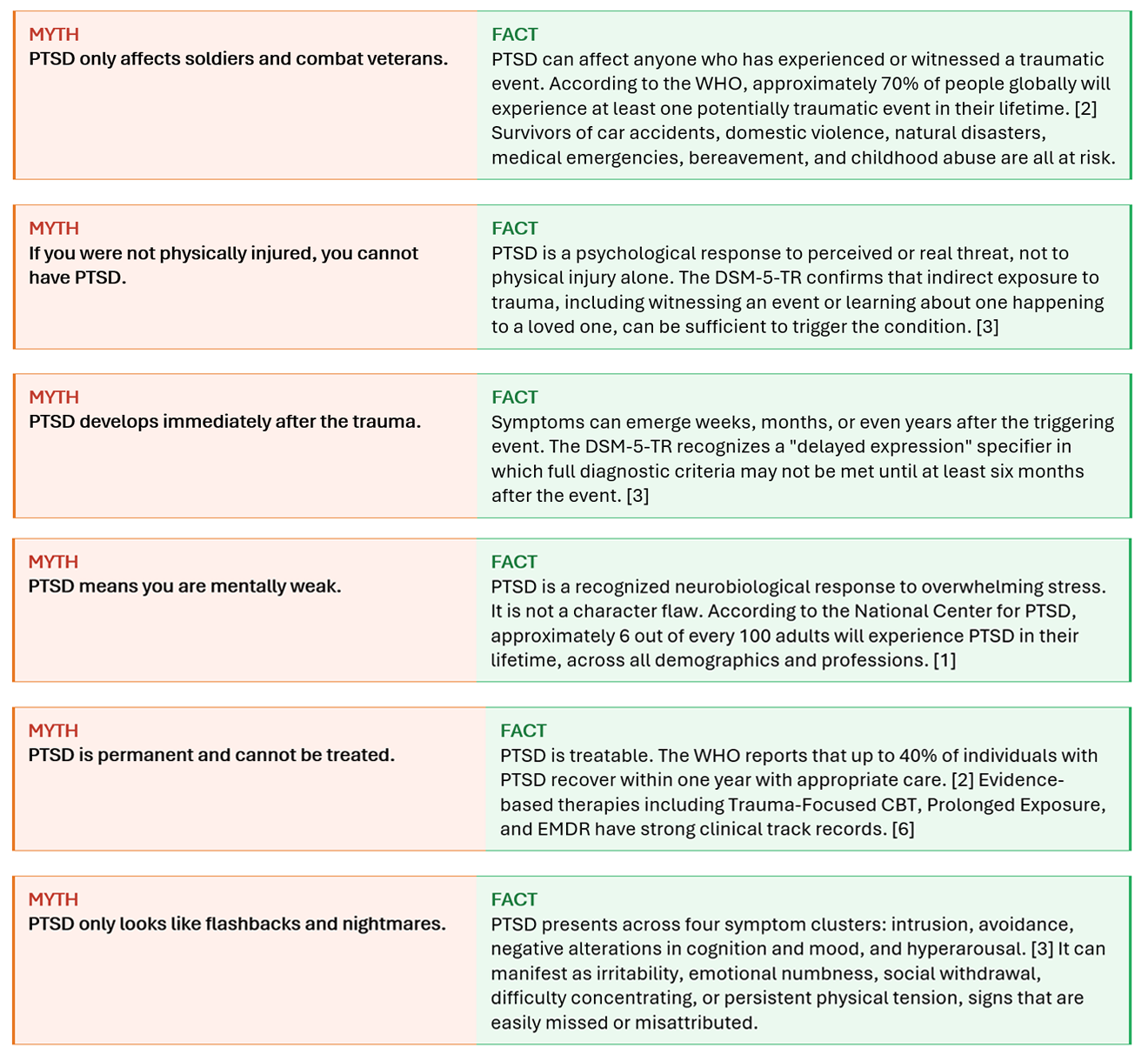
PTSD Affects Anyone, Regardless of Background, Age, or Experience
One of the most critical messages in contemporary trauma research is this: there is no demographic immune to PTSD. It does not discriminate by occupation, social status, gender, age, or prior mental health history. Yet it does not affect everyone equally, and understanding the risk landscape helps identify those who may be suffering in silence.
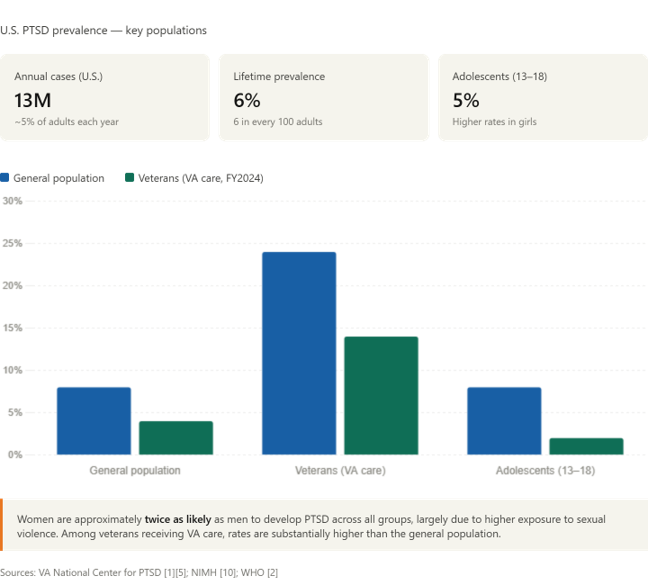
Prevalence Across Populations
In the United States alone, an estimated 13 million Americans are living with PTSD in any given year, representing approximately 5% of the adult population. [1] Across a lifetime, 6 out of every 100 adults will be affected. [1]
Women are approximately twice as likely as men to develop PTSD, a disparity largely related to differential exposure to high-risk trauma types, particularly sexual violence. [1][2] Among veterans, approximately 14% of men and 24% of women receiving VA care carried a PTSD diagnosis in fiscal year 2024. [5]
Children and adolescents are not exempt. The National Institute of Mental Health estimates that 5% of U.S. adolescents aged 13 to 18 have experienced PTSD, with rates notably higher in girls. [10]
How PTSD Can Present Day to Day
PTSD does not always look like Marcus's story. It wears many faces. In a teenager, it may look like angry outbursts and declining school performance. In a new mother, it may look like an inability to bond, driven by a traumatic birth experience. In a first responder, it may look like rigid professional detachment and reliance on alcohol. In an elderly adult, it may look like a sudden worsening of anxiety decades after a long-buried event.
The clinical criteria, as defined by the DSM-5-TR, organize PTSD symptoms into four clusters: [3]
- Intrusion: Unwanted memories, flashbacks, trauma-related nightmares, and intense psychological or physiological distress when reminded of the event.
- Avoidance: Deliberate efforts to avoid thoughts, feelings, people, places, or conversations connected to the trauma.
- Negative cognition and mood: Persistent feelings of shame, guilt, or blame; emotional numbness; detachment from others; loss of interest in previously valued activities.
- Alterations in arousal: Hypervigilance, exaggerated startle response, difficulty sleeping, irritability, and trouble concentrating.
These symptoms must persist for more than one month and cause significant distress or functional impairment to meet the diagnostic threshold. [3] Because so many of these symptoms overlap with depression, anxiety, and burnout, PTSD is frequently misdiagnosed or missed altogether.
"PTSD does not announce itself. It disguises itself as irritability, exhaustion, distance, and a quiet but consuming dread of ordinary things."
The human cost is considerable. Individuals with PTSD are approximately 80% more likely to meet diagnostic criteria for at least one other mental health condition, including major depression, anxiety disorders, or substance use disorder. [3] Depression co-occurs in up to half of all patients. [9] These compounding conditions underscore the urgency of accurate identification and comprehensive care.
Seeking Support Is a Sign of Strength
There is a cultural script that tells us to manage pain privately, to appear unaffected, to get on with it. For individuals living with PTSD, this script is not merely unhelpful. It is harmful.
Choosing to seek help for PTSD is not an admission of weakness. It is an act of courage, and according to the clinical evidence, it is the most effective thing a person can do. The World Health Organization confirms that with the right support, up to 40% of individuals with PTSD recover within a year. [2] Those who engage in evidence-based treatment consistently show better outcomes than those who do not. [9]
Effective Treatment Exists
Current clinical guidelines from the American Psychological Association and the VA/DoD Joint Clinical Practice Guideline recommend the following as first-line interventions for PTSD in adults: [6][8]
- Trauma-Focused Cognitive Behavioral Therapy (TF-CBT), encompassing Cognitive Processing Therapy and Prolonged Exposure therapy, which carry the strongest evidence base currently available. [7]
- Eye Movement Desensitization and Reprocessing (EMDR), a structured intervention endorsed by both the WHO and the APA. [2][6]
- Continual symptom monitoring to track progress, identify setbacks early, and tailor care to the individual.
- Telehealth delivery, which removes geographic and logistical barriers to accessing qualified care, particularly important for those in underserved or rural communities.
Where pharmacotherapy is indicated alongside psychological treatment, evidence supports the use of SSRIs and SNRIs as first-line agents, with close monitoring and regular reassessment by a qualified clinician. [8]
The Barrier That Costs the Most
Despite the availability of these interventions, the WHO estimates that only 1 in 4 individuals with PTSD in lower-resource settings receive any form of treatment. [2] In higher-income settings, stigma, wait times, and lack of awareness remain the most common barriers. The cost of untreated PTSD, measured in fractured relationships, lost productivity, comorbid illness, and preventable suffering, is far greater than the cost of accessing care.
The bravest thing Marcus ever did was walking into that clinic and asking for help.
Today, Marcus sleeps through most nights. He drives again, even when it rains. He still teaches, and he is still the calm one in the staffroom. But now the calm is real.
What made the difference was not willpower. It was not the passage of time. It was structured, evidence-based support delivered consistently and with continuity. It was a system that met him where he was, tracked how he was progressing, and adapted as he did.
That kind of support is no longer confined to a weekly clinic appointment. It is increasingly accessible, and for many people, it begins with a single question: what if I reached out?
What Support That Meets You Where You Are Looks Like
Marcus did not recover because he found the perfect therapist on the first try. He recovered because once he had access to the right tools, the process of understanding his own patterns became less opaque. He could see what was happening. He could track when things were improving and when they were not. He had structured conversations that moved him forward rather than simply sitting with what he had already experienced.
Syrenity, developed by SyraHealth, is built around exactly that kind of support. It is a mental and behavioral health platform grounded in clinical evidence, designed not as a substitute for care but as a continuous, accessible companion to it.
For Someone Like Marcus, and the Millions Like Him
- Scientific Assessments: Marcus spent eighteen months wondering whether what he felt was real. Validated clinical screening tools remove that uncertainty, providing an evidence-based picture of what is actually present and how severe it is.
- Continual Monitoring: Recovery from PTSD is not linear. Syrenity tracks mood, symptoms, and functional wellbeing over time, so that changes, both improvements and setbacks, are visible and can be responded to early.
- Cognitive Behavioral Therapy (CBT): The same structured therapeutic approach that the APA and VA/DoD identify as the strongest evidence-based treatment for PTSD [6][8] is available through the platform, guided and purposeful.
- Telehealth: For anyone who has ever told themselves that finding the time, the access, or the courage to sit in a waiting room is too much, Syrenity removes that specific barrier entirely.
- And more: An integrated continuum of mental and behavioral health support, from first recognition through sustained recovery, in one place.
- Marcus's story did not end with a diagnosis. It began there.
- Yours does not have to end with silence.
Page References
All sources cited in this article are listed below. Online resources were verified and accessed in June 2026.
[1] U.S. Department of Veterans Affairs, National Center for PTSD. "How Common Is PTSD in Adults?" VA.gov. Accessed June 2026. https://www.ptsd.va.gov/understand/common/common_adults.asp
[2] World Health Organization. "Post-Traumatic Stress Disorder (PTSD)." WHO Fact Sheet. May 2024. https://www.who.int/news-room/fact-sheets/detail/post-traumatic-stress-disorder
[3] American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Washington, DC: APA; 2022.
[4] Hathorn JR, et al. "National Trends in PTSD Among US Military Veterans: 2025-2026 NHRVS." Journal of Clinical Psychiatry. 2025.
[5] U.S. Department of Veterans Affairs, National Center for PTSD. "How Common Is PTSD in Veterans?" VA.gov. Accessed June 2026. https://www.ptsd.va.gov/understand/common/common_veterans.asp
[6] American Psychological Association. "Clinical Practice Guideline for the Treatment of PTSD in Adults." APA; 2024. https://www.apa.org/ptsd-guideline/ptsd.pdf
[7] American Psychological Association. "CE Corner: PTSD and Trauma: New APA Guidelines." APA Monitor on Psychology. July/August 2025.
[8] VA/DoD Clinical Practice Guideline Working Group. "The Management of PTSD and Acute Stress Disorder." VA & DoD CPG; 2023 (updated 2024).
[9] Ricciardi L, et al. "Posttraumatic Stress Disorder: Evaluation and Treatment." American Family Physician. 2023;107(3).
[10] National Institute of Mental Health (NIMH). "Post-Traumatic Stress Disorder." NIMH.nih.gov. Accessed June 2026.