

Healthcare Disparities: Why Millions Still Fall Through the Cracks
What They Are. Why They Matter. How to Fix Them.
Wake Up Call: Today's Numbers
Right now, as you read this:

¹ SAMHSA 2024 | CDC WISQARS 2024 | SAMHSA Economic Analysis 2024
Here's What Healthcare Disparities Look Like in 30 Seconds
"Two people walk into a doctor's office with the same problem. One leaves with a diagnosis and treatment plan. The other leaves confused, with a six-month waitlist, and no follow-up. One recovers. The other suffers quietly for years. The gap? That's a healthcare disparity."
It's not about bad doctors. It's about broken systems. And the systems are broken in ways that hurt some groups much more than others.
Still confused? Let's break it down.
What Are Healthcare Disparities, Actually?
Official definition (the boring way):
"Healthcare disparities are differences in incidence, prevalence, mortality, and burden of diseases and other adverse health conditions that exist among specific population groups."
— National Institute on Minority Health and Health Disparities (NIMHD)¹
Translation (the real way):
Some groups of people get sick more often, stay sick longer, die younger, and suffer more—not because of bad luck or bad genetics, but because of how healthcare is organized and who has access to it.
Breaking Down the Definition: 4 Parts
That official definition hides four critical ideas. Here they are:
-
INCIDENCE: How many NEW cases show up
Example: Type 2 Diabetes (2024)

Translation: Black Americans are getting diabetes at nearly 2x the rate. Not because they're less healthy—but because they have less access to preventive care, more food insecurity, and more stress.² That's a disparity in incidence.
2. PREVALENCE: How many people CURRENTLY have it
Example: Mental Illness (2024)
 Mental health disparities in treatment access: A SAMHSA survey reveals that while White Americans report higher diagnosed mental illness rates (25% vs 21%), the starkest gap emerges in treatment-seeking. The 'Getting Help' column exposes a troubling reality: access to care is not equally distributed.³
Mental health disparities in treatment access: A SAMHSA survey reveals that while White Americans report higher diagnosed mental illness rates (25% vs 21%), the starkest gap emerges in treatment-seeking. The 'Getting Help' column exposes a troubling reality: access to care is not equally distributed.³
3. MORTALITY: How many people DIE
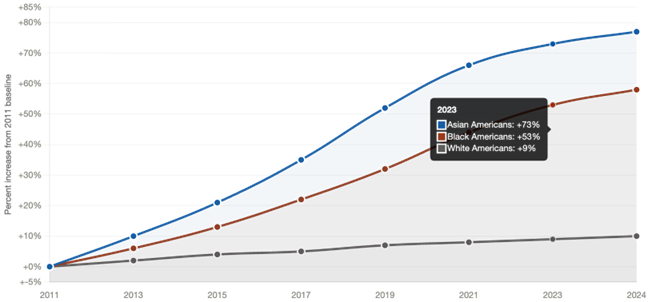
Example: Suicide & Mental Health Deaths (2024) — The Accelerating Crisis
 As per Suicide mortality data (2024): While White American suicide rates are rising slowly, rates among people of color are skyrocketing. ⁴
As per Suicide mortality data (2024): While White American suicide rates are rising slowly, rates among people of color are skyrocketing. ⁴
4. BURDEN: How much total suffering happens
Time sick. Money lost. Disability. Missing work. Not getting better. The full human cost. Example: The Treatment Gap (2024)
 That's 6.4 million Black Americans with mental illness who aren't getting help. That's not a statistic. That's a person in your community, your neighbor, your family member, suffering in silence.
That's 6.4 million Black Americans with mental illness who aren't getting help. That's not a statistic. That's a person in your community, your neighbor, your family member, suffering in silence.
That's the burden.⁵
Why Do Disparities Exist? (The Real Talk)
Spoiler alert: It's not genetics. It's not culture. It's not laziness. It's structure.
The Five Biggest Barriers (2024 Data)
Barrier 1: You Can't Afford It
 16.4% of Hispanic Americans are uninsured. That's more than 2.5x the rate for White Americans. Average therapy
16.4% of Hispanic Americans are uninsured. That's more than 2.5x the rate for White Americans. Average therapy
= $100-250/session.⁶
Barrier 2: There's No One There
Mental health providers per 100,000 people:
- White neighborhoods: 45 providers (wait: 3-4 weeks)
- Black neighborhoods: 12 providers (wait: 8-12 weeks)
- Hispanic neighborhoods: 8 providers (wait: 12+ weeks)⁷
Barrier 3: The Provider Doesn't Look Like You

Only 4% of psychologists are Black. That means 96% of Black patients seeking a Black therapist have no option. Studies show culturally matched care = better outcomes.⁸
Barrier 4: Cost Is a Deal-Breaker
Among people who needed mental health care but didn't seek it:

Cost is the #1 barrier. It disproportionately hits communities of color because of income gaps, unemployment, and underinsurance.⁹
Barrier 5: You Don't Know Where to Start
24% of Hispanic Americans who needed mental health care said they didn't know how to find a provider. For comparison: Only 11% of White Americans have said the same. That's a navigation gap. A system that's designed for people who already know how to navigate it.¹⁰
How Do We Fix This?
Good news: Disparities aren't inevitable. They're not unsolvable. Research shows what actually works.
Five Evidence-Based Solutions
Solution 1: Measure What Matters
Organizations that track disparities by race, ethnicity, and neighborhood can see exactly where gaps are. Real-time dashboards help catch problems early and adjust fast. You can't fix what you don't measure.
Solution 2: Make Care Accessible
Community health centers, telehealth, digital tools that work 24/7. People shouldn't have to wait 3 months or drive an hour for help. Digital behavioral health platforms can reach people where they already are.
Solution 3: Build a Diverse Workforce
Training and hiring more mental health professionals who are Black, Hispanic, Asian, and from other communities of color. Recruitment programs that identify talent early. Retention support. This is long-term work, but it's critical.
Solution 4: Partner with Communities
Peer navigators. Community health workers. People from the community who understand the barriers and can guide others through the system. Trust matters. Systems designed with communities, not for them, actually work.
Solution 5: Remove Barriers
Sliding-scale fees. Telehealth. Transportation support. Language services. Education about where to go and how to get there. If you remove cost, time, distance, and confusion—people use services more.
Programs that combine all five of these show the biggest improvements in outcomes and the fastest reduction in disparities.
What Does This Look Like in Practice?
Here's where organizations actually do this work:
Example 1: Real-Time Equity Analytics
A health system discovers through data analysis that Black patients have a 3-month longer wait time for psychiatric appointments than White patients. They investigate, find staffing gaps in Black neighborhoods, hire 2 new providers there, and set a goal to equalize wait times. Six months later: wait times are equal across all neighborhoods. Without measurement, this disparity would have stayed invisible.
Example 2: Digital Access + Community Outreach
A public health agency launches a digital mental health platform designed for underserved communities. They partner with trusted community organizations to promote it, offer peer navigation, and provide tablets to patients without smartphones. They provide multilingual support. Result: 40% increase in screening, 25% increase in treatment initiation within 6 months.
Example 3: Integrated Workforce Development
An organization works with universities to identify and support students of color pursuing mental health degrees. They provide mentorship, placement, and loan forgiveness. They recruit community health workers from the neighborhoods they serve. Over 3 years, they go from 8% of their clinical staff being Black to 22%.
The Bigger Picture:
Organizations solving disparities need partners who understand both the clinical side and the operational side. They need tools that work together—not separately.
They need:
- Real-time analytics that show where disparities are
- Digital tools that reach people where they are
- Community partnerships built into the system
- Education and outreach that builds trust
- Workforce support to build a diverse provider base
This is exactly what Syra Health is built to do—combining health equity analytics, population health management, digital behavioral health, community outreach, and workforce development to improve health outcomes. These tools don't work separately. They work together.
References
¹ SAMHSA (2024). Results from the 2021-2023 National Survey on Drug Use and Health. Center for Behavioral Health Statistics and Quality. CDC (2024). WISQARS Database. Youth Risk Behavior Surveillance System.
² CDC (2024). Health Disparities & Inequalities Report. Division of Diabetes Translation. U.S. Census Bureau (2024). American Community Survey: Food Insecurity Data.
³ SAMHSA (2024). Behavioral Health by Race and Ethnicity: Results from the 2021-2023 NSDUH. KFF (2024). Racism, Discrimination and Health Survey.
⁴ CDC WISQARS (2024). Suicide Mortality Data. Analysis of trends 2011-2024 across racial and ethnic groups.
⁵ KFF (2024). Racial and Ethnic Disparities in Mental Health Care. Survey data showing treatment gaps across populations.
⁶ U.S. Census Bureau (2024). American Community Survey. Insurance coverage by race and ethnicity.
⁷ NIMHD (2024). Health Professional Shortage Area Database. Mental health provider distribution analysis.
⁸ American Psychological Association (2024). Demographic Statistics of U.S. Psychologists. Bureau of Labor Statistics occupational data.
⁹ KFF (2024). Racism, Discrimination and Health Survey. Primary barriers to mental health care access.
¹⁰ KFF (2024). Barriers to Mental Health Care. Navigation and awareness analysis.
All data from official U.S. government and peer-reviewed sources. Visit syrahealth.com for health equity solutions.